Understanding the Mini Gastric Bypass vs Roux-en-Y difference is crucial for patients navigating bariatric surgery options. A common misconception is that the “Mini” Gastric Bypass (MGB) is a minor or less effective procedure; in reality, it is a powerful metabolic intervention that often results in greater weight loss than the traditional method. At Clinic Care Center, we offer both procedures, tailoring the choice strictly to your metabolic health, anatomy, and history of acid reflux.
Anatomy 101: One Anastomosis (MGB) vs. Two (RNY)
The primary distinction lies in how the surgeon reconstructs the digestive tract. The Roux-en-Y Gastric Bypass (RNY) is the traditional method involving two connections (anastomoses): one to the pouch and one lower down the intestine. This “Y” shape creates a barrier that diverts bile away from the stomach, effectively curing acid reflux.
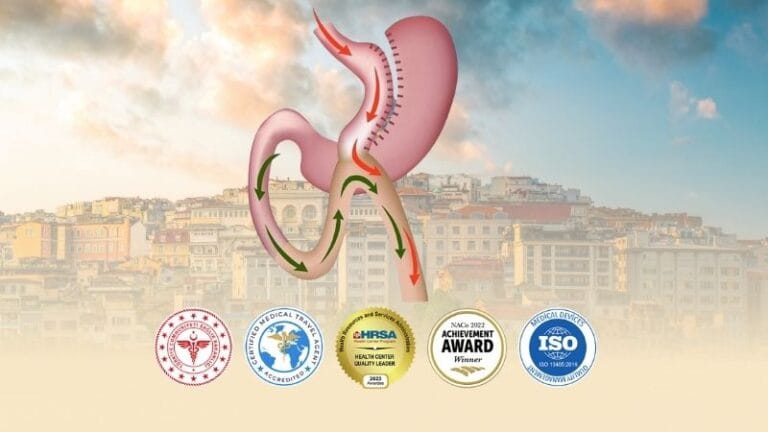
Conversely, the Mini Gastric Bypass (MGB), also known as One Anastomosis Gastric Bypass (OAGB), involves only one connection. The surgeon creates a long, tube-like pouch and loops the small intestine up to it. While this technique is faster to perform, it creates a longer bypass of the small intestine (approximately 150-200cm), leading to significant malabsorption of calories and nutrients.
Clinic Care Center: The Critical “Reflux” Warning
The decision between Mini Bypass and Roux-en-Y is often determined by one major factor: Acid Reflux (GERD). If you have a history of severe heartburn or Barrett’s Esophagus, Mini Gastric Bypass is generally contraindicated because it carries a risk of ‘Bile Reflux’ (bile flowing back into the stomach). In these cases, Roux-en-Y is the Gold Standard as it physically stops reflux. At Clinic Care Center, we perform a mandatory endoscopy to check your stomach health before recommending the Mini Bypass.
Head-to-Head Comparison: MGB vs. RNY
To help you understand the trade-offs between these two major surgeries, we have compiled a direct comparison of their features and expected outcomes.
| Feature | Mini Gastric Bypass (MGB/OAGB) | Roux-en-Y Gastric Bypass (RNY) |
|---|---|---|
| Connections (Anastomosis) | 1 (Single Loop) | 2 (Y-Shape) |
| Operating Time | Shorter (45-60 mins) | Longer (90-120 mins) |
| Excess Weight Loss (18 Months) | High (70% – 80%) | High (65% – 75%) |
| Reflux (GERD) Impact | Risk of Bile Reflux | Cures Acid Reflux |
| Vitamin Deficiency Risk | Higher (More Malabsorption) | Moderate |
| Reversibility | Easier to Reverse | Difficult/Complex |
Recovery Timeline & Nutritional Risks
Both surgeries require a strict liquid diet for 2-3 weeks post-op to allow the staple lines to heal without pressure. However, the long-term risks differ. Mini Gastric Bypass patients typically have lower iron and calcium levels due to the bypassed intestine length. Lifetime commitment to bariatric multivitamins is non-negotiable for both, but even stricter for Mini Bypass patients to prevent anemia and osteoporosis.
Frequently Asked Questions (FAQ)
Is Mini Gastric Bypass cheaper?
Generally, the Mini Gastric Bypass is slightly more cost-effective because it requires less operating room time and fewer surgical cartridges (staplers) than the Roux-en-Y.
Which surgery cures Type 2 Diabetes better?
Both surgeries are excellent for inducing remission of Type 2 Diabetes. However, clinical data suggests the Mini Gastric Bypass has a slightly stronger metabolic effect due to the greater malabsorption.
Can I switch from Sleeve Gastrectomy to Bypass?
Yes. If a Sleeve Gastrectomy patient develops severe reflux or regains weight, converting to a Roux-en-Y Bypass is a common and effective revision strategy.
What is Dumping Syndrome?
Dumping Syndrome occurs when sugar moves too quickly from the stomach to the small intestine, causing nausea, dizziness, and sweating. It occurs in both procedures and acts as a deterrent against eating sweets.
Does Mini Bypass cause stomach cancer?
There has been theoretical concern that bile reflux in MGB could lead to cellular changes. However, long-term studies have shown this risk is extremely low. We mitigate this by selecting the right patients and ensuring the connection is made low enough in the intestine.
How much weight will I lose?
While individual results vary based on lifestyle adherence, patients typically lose between 65% to 80% of their excess body weight within the first 18 months.
Which Surgery is Right for You?
Choosing between MGB and RNY is a medical decision, not just a preference. Your history of reflux, diabetes status, and lifestyle determine the safest option. Contact the bariatric team at Clinic Care Center for a comprehensive evaluation and a personalized surgical plan.
Also Read:
Gastric Sleeve in Turkey
Gastric Bypass in Istanbul Turkey
Gastric Balloon in Istanbul, Turkey